Root Causes is a policy analysis series by the Natrona Collective Health Trust, grounded in rigorous, nonpartisan research. Each installment examines the systems, data, and decisions that shape the health and well-being of Natrona County residents by going beyond the headlines to understand why things are the way they are, and what it means for the people who live here. We believe an informed community is a healthier one. If you have a topic suggestion or question, reach out to Rachel Bouzis, Director of Policy & Learning.
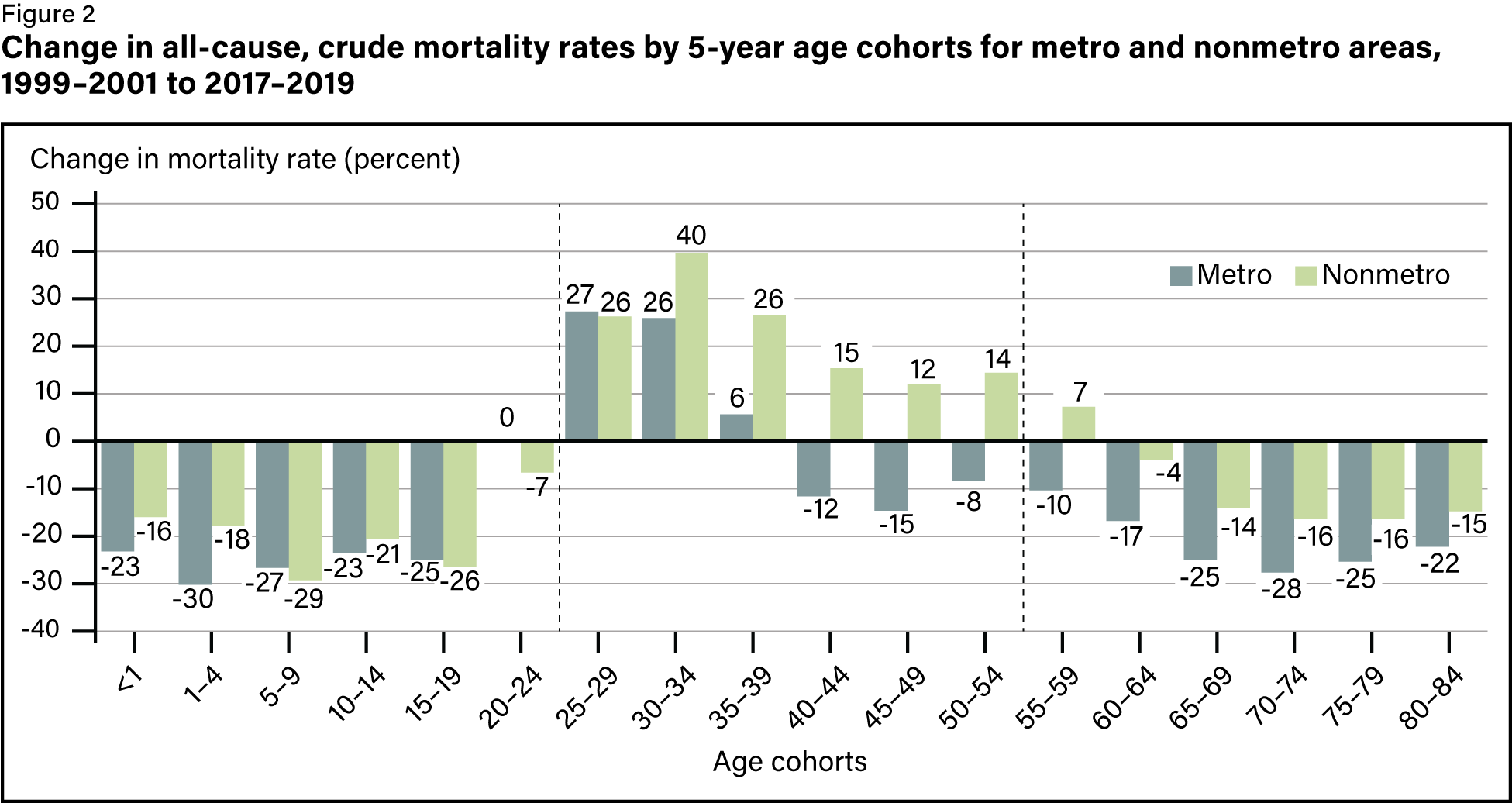
The nostalgia for rural America doesn’t seem to take into account that it’s dying faster than urban America. A 2024 USDA report found that disease-related deaths among adults ages 25 to 54 were a staggering 43% higher in rural areas than in urban areas in 2019, up from just 6% higher in 1999. As urban areas have lowered natural causes morbidity rates, rural areas have worsened—significantly.
Even more troubling is how stark these disparities are becoming for women and Indigenous peoples, especially Indigenous women. The 25-to-54 age range is designated prime working age, or when we should at least be healthy enough to work. Unfortunately, over the last 25 years, we’ve been trending in the wrong direction.
How we got here
Mortality rates across metropolitan and nonmetropolitan areas had been an area of concern as early as 1990, but this initial research included both external causes of death—suicides, overdoses, accidents, violence, etc.—and natural causes of death—cancer, heart disease, respiratory disease, etc. The 2024 study examines external causes and natural causes of mortality, or NCM, separately, focusing on prime working ages.
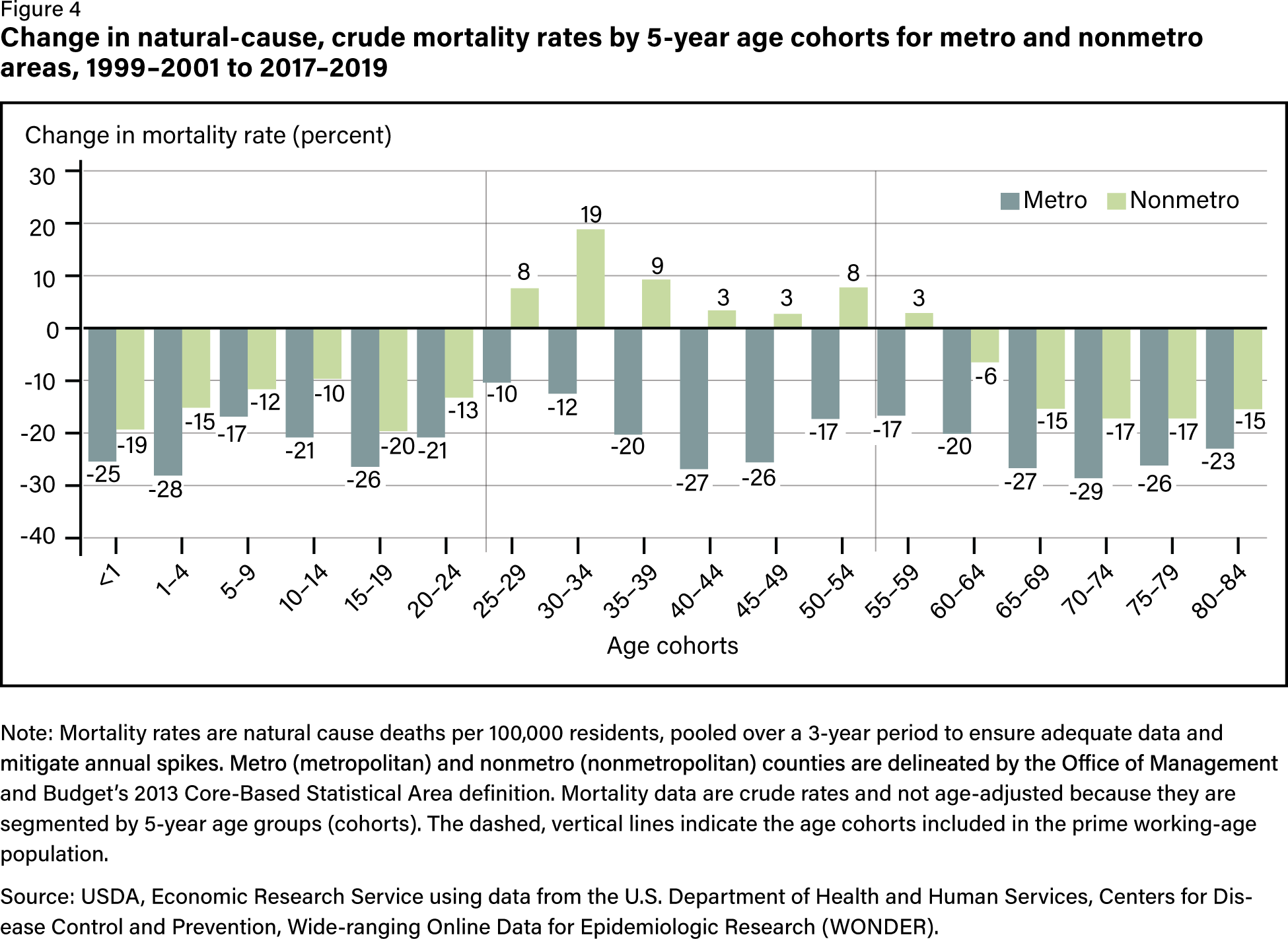
From 1999 to 2019, the prime working age NCM gap between urban and rural areas jumped by 51 deaths per 100,000 residents. Urban areas lowered this rate by 37 percent as it increased in rural areas by 14 percent. Notably, the more rural the area, the greater the increase in NCM. Furthermore, female prime working age NCM rates grew by 16 percent over that time compared to 2 percent for males. The highest rate of NCM growth for rural women was pregnancy-related deaths, which grew by 313 percent.
Rural women are more than 60 percent more likely to die from pregnancy than urban women.1
It’s also worth noting that nationwide, Black women are three times more likely to die from pregnancy than white women with 49.4 deaths per 100,000 births compared to just 14.9.2
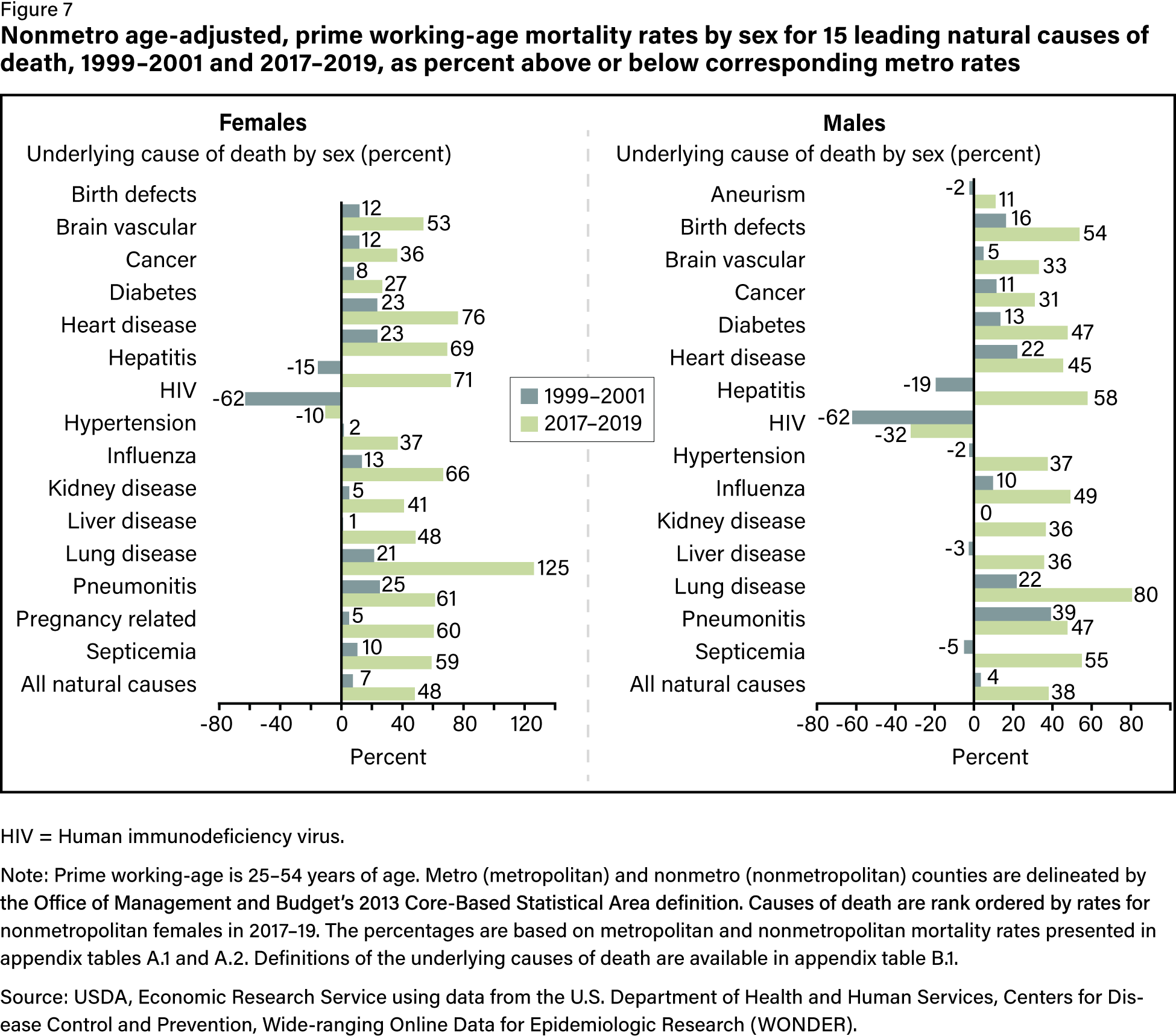
Indigenous peoples experience some of the poorest health outcomes, and they’re even graver in rural areas. There was a 39 percent increase in NCM prime working age males and 55 percent increase for Indigenous women.
The compounding burden
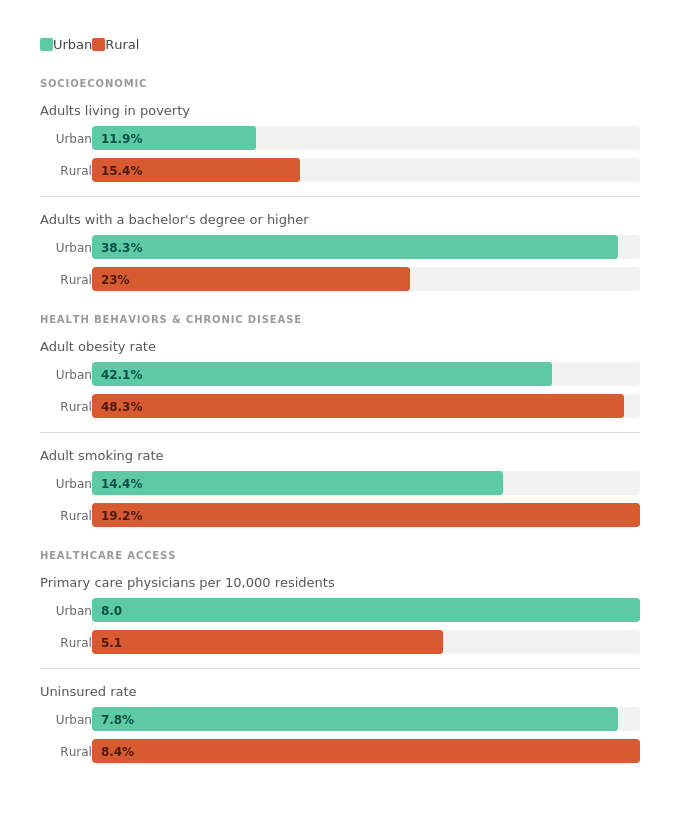
The factors driving this gap aren’t a mystery. Rural America carries a compounding burden across nearly every social and health indicator, and the deficits reinforce each other. Lower education and higher poverty feed higher rates of chronic disease, which feed higher mortality. And the health care system built to interrupt that cycle is stretched thinnest exactly where the need is greatest.
A $50 billion band-aid
Clearly, rural health needs transformed. What’s also becoming clear is that the Rural Health Transformation Plan is unlikely to do so. The 2025 budget reconciliation bill cut an estimated $911 billion from federal Medicaid spending and the Affordable Care Act marketplace. KFF estimates that just Medicaid reductions could be $137 billion over ten years in rural areas.3 This was why $50 billion in funding over five years was added to that bill as the Rural Health Transformation Program.
I guess we need to first state the obvious: $50 billion is a lot less than $137 billion. States can use just 15 percent of their allocations to pay providers for patient care and prohibits capital construction in most cases. The Centers for Medicare and Medicaid Services director, Dr. Mehmet Oz, said these funds are to “not to pay operating expenses,” but instead “right-size the system and to deal with the fundamental hindrances of improvement in rural health care.” The administration expects states to accomplish this through technology, which is where the vast majority of this money will be spent.4
Also obvious but evidently needs explanation: the proficiency of a hospital’s technology is irrelevant if a hospital is closed. I wrote about how low patient volume and high fixed costs make rural healthcare more of a gamble than an investment. Since 2005, nearly 200 rural hospitals have completely or partially closed, and more than 400, more than 20 percent of all rural hospitals, are at risk of closure.5 To fire a flare into a minefield, nearly 1 in 4 people in rural areas are covered by Medicaid. The program being decimated by this same bill is essential to keeping rural hospitals open. This software had better be good.
A map of rural health fund allocations looks almost nothing like a map of rural need. The law requires that half of all funds are distributed equally across approved states—no matter what. This means that though large rural states like Texas, Alaska, and California received the biggest awards, the spending per rural resident is dwarfed by predominantly urban states like Massachusetts and New Jersey. Texas is receiving just $66 dollars per rural resident while Rhode Island gets a whopping $6,305.6
Moreover, as we’ve learned, rural healthcare needs are not neatly distributed. States with the lowest rural mortality rates have been awarded about twice as much funding per rural resident than states with the highest rural mortality rates. States most at risk, like Mississippi, Kentucky, and Tennessee, will receive an average of $104 per rural resident compared to states with better health outcomes like Connecticut and Vermont, which average $233 per rural resident.7
The math doesn’t add up
According to KFF, “it is highly unlikely that any state will receive more money from the rural health fund than it will lose from the historic cuts to federal funding for health care.”8 Wyoming, as a nonexpansion and almost entirely rural state, was initially projected to be the nation’s largest beneficiary of rural health funds.9 But as of late April, Wyoming’s rural health fund dollars are in red tape limbo. The state’s application, along with Colorado and West Virginia, is still under CMS review.
What this means for families
As a new mom, I find the life-threatening dangers of pregnancy—of having a family—in rural America shameful. In the last five years, more than 100 rural hospitals have closed labor and delivery units.10 Nearly 50 percent of all births in rural communities are covered by Medicaid.11 To recap, we gutted the system that was barely keeping hospitals afloat by nearly one trillion dollars. The innovative, once-in-a-lifetime solution to this problem? Give $50 billion back.
“Rural Health Transformation will not save a single hospital in our state. I don’t think it will save a single hospital nationally,” the director of the Nebraska Rural Health Association said. It seems unlikely, then, that it will save any of those rural Americans who are dying at tragically young ages at a much faster rate than their urban counterparts. It’s all but certain to increase mortality rates for rural women due to pregnancy. I shudder to think how high that ceiling will get for Black and Indigenous women.
We need to know why rural Americans are dying younger than they should, so we must demand that government invests in research like the USDA report. We need to keep hospitals open, so we must demand that our government fund Medicaid. We need Americans to live longer, healthier lives, so we must demand that our government actually transforms rural health care.
Sources
- Urban-rural differences in pregnancy-related deaths, United States, 2011–2016 ↩
- Racial Disparities in Maternal and Infant Health: Current Status and Key Issues ↩
- Comparing States’ Rural Health Fund Allotments to Medicaid Spending Cuts Can Be Misleading ↩
- Here’s what to know about the $50 billion states are getting for rural health ↩
- Why Rural Hospitals Are Facing A Funding Crisis – And How It Could Get Worse ↩
- First-Year Rural Health Funds Awards Range From Less than $100 Per Rural Resident in Ten States to More than $500 in Eight ↩
- Analysis of the Rural Health Transformation Program ↩
- Comparing States’ Rural Health Fund Allotments to Medicaid Spending Cuts Can Be Misleading ↩
- State-Level Impacts of Key Medicaid Provisions in the One Big Beautiful Bill Act ↩
- Positive Outliers: How Some Rural Communities Maintain Access to Labor and Delivery Services ↩
- Fact Sheet: Medicaid ↩
- Rural Poverty & Well-Being ↩
- Educational attainment in rural America rises, but urban areas widen the degree gap ↩
- The Urban-Rural Digital Divide in Internet Access and Online Activities During the COVID-19 Pandemic ↩
- Chronic health conditions and healthcare affordability issues among U.S. rural and urban adults ↩
- U.S. Obesity Rate Changes Differ for Rural and Urban Areas, as Well as Across Regions ↩
- Trends in Rural and Urban Cigarette Smoking Quit Ratios in the US From 2010 to 2020 ↩
- Availability of healthcare providers in rural areas lags that of urban areas ↩
- Health Insurance Coverage in Rural and Urban Areas in the U.S., 2023 ↩
Recent Posts
-
 We spend $17 million a year. Not all of it goes where you think.
We spend $17 million a year. Not all of it goes where you think. -
 We used to let the work speak for itself. That wasn’t enough.
We used to let the work speak for itself. That wasn’t enough. -
 In Name Only: The Rural Health Transformation That Isn’t
In Name Only: The Rural Health Transformation That Isn’t -
 Nothing To See Here: Above the Board Dark Money at Your Expense
Nothing To See Here: Above the Board Dark Money at Your Expense -
 The Gloves Don’t Fit: The Invisible Hand and Rural Health Care
The Gloves Don’t Fit: The Invisible Hand and Rural Health Care